Murphy Endotracheal Tube
The “Murphy eye” is the eponymous name for a hole on the side of most endotracheal tubes (ETTs) that functions as a vent, and prevents the complete obstruction of the patient’s airway, should the primary distal opening of an ETT become occluded.
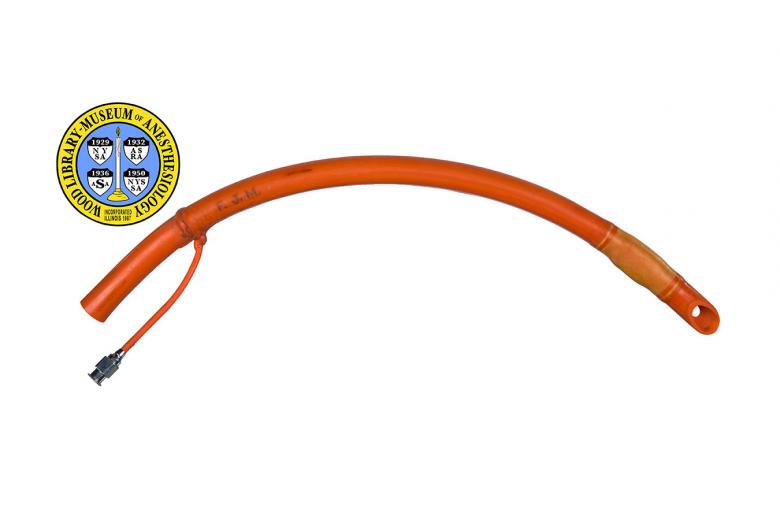
Dr. Francis J. Murphy (1900-1972) was an outspoken proponent of the need for continuous oxygen supply during anesthesia. In 1941, he laid down the nine characteristics of the "ideal" endotracheal tube (ETT.) In the same article he described two tubes with characteristics new to ETT design. One of the tubes was straight with two side holes and the other was curved with one side hole. Both were without cuffs. They were made of a high quality red rubber stock that balanced flexibility and resistance to compression or kinking even after numerous uses and heat sterilizations. Although most ETTs used today are made of disposable plastic they still need to balance flexibility and resistance to compression, and most continue to incorporate the important safety feature that bears Dr. Murphy's name.
This example of the tube was owned by Dr. Murphy himself, and bears his initials. It has an inflatable cuff above the "eye". The cuff is inflated through the small side tube that is attached to the wall of the endotracheal tube. When inflated, the cuff helps to prevent aspiration.
Catalog Record: Murphy Endotracheal Tube
Access Key: akgw
Accession No.: 2011-02-10-1 B
Title: [Murphy endotracheal tube] : 38 / [designed by Francis John Murphy.]
Author: Murphy, Frank J. (Francis John), 1900-1972.
Corporate Author: Foregger Company.
Title variation: Alt Title
Title: Murphy eye.
Title variation: Alt Title
Title: Murphy intratracheal catheters.
Title variation: Alt Title
Title: Murphy tube.
Publisher: West Germany : Foreggor, [1950-1975].
Physical Descript: 1 endotracheal tube : rubber, metal : 7.5 x 1.5 x 27 cm
Subject: Airways.
Subject: Intubation, Intratracheal – instrumentation.
Subject: Anesthesia, Intratracheal.
Subject: Airway Management Equipment.
Note Type: General
Notes: Title based on common name for the object; Early possible date of manufacture
(1950) based on mark of “West Germany” on object, and that the 1949 Foreggor
catalog does not contain the Murphy ETT in it, but the 1952 Foreggor catalog
does; Late possible date of manufacture (1975) based on the inventer initials
on tube (F.J.M.) and the year of Dr. Murphy’s death. The date range could
change if documentation indicates the range should be corrected.
Note Type: Citation
Notes: Forestner JE. Frank J. Murphy, M.D., C.M., 1900-1972: his life, career and
the Murphy eye. Anesthesiology. 2010;113(5):1019-1025.
Note Type: Citation
Notes: Maltby JR. Murphy eye: Francis John Murphy (1900-1972). In: Notable Names in
Anaesthesia. London: Royal Society of Medicine Press; 2002:151-153.
Note Type: Citation
Notes: Murphy FJ. Two improved intratracheal catheters. Anesth Analges.
1941;20(2):102-105.
Note Type: Citation
Notes: Tamakawa S. Every endotracheal tube needs a Murphy eye! Can J Anaesth. 1999
Oct;46(10):998-999.
Note Type: Physical Description
Notes: One red rubber endotracheal tube with a rounded, beveled distal end and a
oval hole cut into the side on the side opposite the beveled opening;
Measured end to end in a straight line, the length is approximately 27 cm;
Measured end to end along the curve, the length is approximately 31 cm; There
is a cuff located above the eye, and a metal inflation port approximately 5.5
cm below the proximal end; the port is at the end of an approximately 6 cm
inflation tube; The initials “F. J. M.” are written in ink approximately 7 cm
below the proximal end; Manufacturers markings on tube are faded and include,
“FOREGGOR 38”, and “WEST GERMANY”.
Note Type: Reproduction
Notes: Photographed by Mr. Steve Donisch on January 14, 2013.
Note Type: Acquisition
Notes: Donated to the WLM by the family of Dr. Frank J. Murphy.
Note Type: Historical
Notes: The “Murphy eye” is the eponymous name for a hole on the side of most
endotracheal tubes (ETTs) that functions as a vent, and prevents the complete
obstruction of the patient’s airway, should the primary distal opening of an
ETT become occluded. The distal opening can become blocked by contact with
the wall of the trachea or bronchi, or by tissue masses, blood clots or mucus
plugs. It is located very near, and on the wall opposite, the beveled distal
opening.
Note Type: Historical
Notes: Dr. Francis John Murphy (1900-1972) preferred to be called Frank. He had
roots in both the United States and Canada. Born in South Dakota, his family
moved to Alberta when he was 11. Dr. Murphy earned his medical degree from
McGill University in 1925, and for the succeeding five years spent most of
his time working in Montreal. In 1930 he moved to Detroit to take the
position of Chief of Anesthesia at Harper Hospital. He was there until 1942,
when he enlisted in the United States Navy to serve during World War II. In
1941 Dr. Murphy published an article titled, “Two Improved Intratracheal
Catheters,” in which he described two endotracheal tubes (ETTs) with
characteristics new to ETT design. One of the tubes was straight with two
side holes and the other was curved with one side hole. Both were without
cuffs. Not only did they incorporate the side holes he referred to as “eyes,”
they were made of a high quality red rubber stock that balanced flexibility
and resistance to compression or kinking even after numerous uses and heat
sterilizations. Flexibility and resistance to kinking and compression were
three of nine characteristics of “the ideal” ETT laid down by Dr. Murphy in
his 1941 article. Although most ETTs used today are made of disposable
plastic they still need to balance flexibility and resistance to compression,
and most continue to incorporate the important safety feature that bears his
name: The Murphy eye.
Note Type: Publication
Notes: Ho AM, Wan IY, Wong RH, Ng CS, Ng SK. Provision of stable lung isolation in
an unstable patient: an endobronchial blocker through the Murphy eye of the
in situ endotracheal tube. J Anesth. 2011 Jun;25(3):454-456.
Note Type: Publication
Notes: Krzanowski TJ, Mazur W. A complication associated with the Murphy eye of an
endotracheal tube. Anesth Analg. 2005 Jun;100(6):1854-1855.
Note Type: Publication
Notes: Mphanza T, Jacobs S, Chavez M. A potential complication associated with
percutaneous tracheostomy with an endotracheal tube with a Murphy eye in situ
Anesthesiology. 1998 May;88(5):1418.
Note Type: Exhibition
Notes: Chosen for the WLM website (noted April 2, 2013).
